
Imagine this scenario: Three laps to go, you're in a podium position. The tires are warm, the line is perfect – and then it starts. First a slight tingling in your right forearm. Five minutes later your arm is as hard as concrete and you can barely feel the brake lever. The final laps are no longer a matter of strategy but pure damage control.
That is exactly what happened to Fabio Quartararo at Jerez in 2021. His own words describe it perfectly: "I had to brake with four fingers and normally I brake with one. I couldn't go full gas on the straight. No more power. It was dangerous for me to ride the half race but I didn't want to stop." Jack Miller could simply no longer feel his front brake lever for the last four laps of that same race. And Casey Stoner reportedly lost 95% of the strength in his right arm at the 2010 Dutch TT.
Arm pump is so ubiquitous in MotoGP that the scars on riders' forearms are considered a rite of passage. When all published studies are combined, motorcycle riders account for 66% of all documented CECS cases worldwide – more than all other sports combined (Hirardot et al., OTSR, 2024).
The good news: Arm pump is not fate. It is a metabolic and structural problem – and both can be directly influenced with the right training.
What Is Arm Pump, Really? The Pathophysiology Explained
Arm pump is the colloquial term for Chronic Exertional Compartment Syndrome (CECS) of the forearm. Behind this unwieldy medical name lies a mechanistic problem that can be explained quite logically.
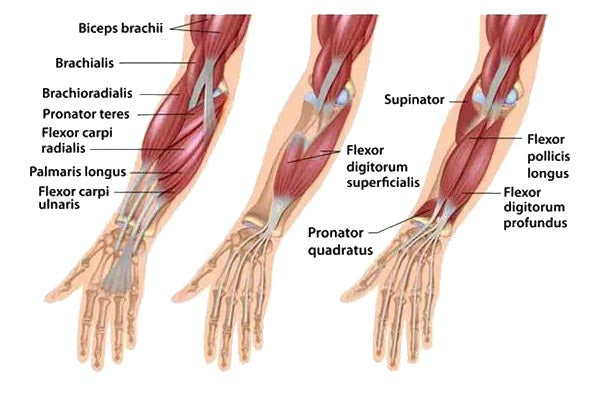
Your forearm is divided into four compartments – muscle groups each enclosed by a fascia. This fascia is a tough connective-tissue sheath that barely stretches. While you ride, your muscles demand more blood: arterial inflow increases dramatically, and the muscle tissue can swell by up to 20% of its resting volume (Chandwani & Varacallo, StatPearls, 2023).
As long as the fascia is elastic enough, no problem. But that is exactly the crux: in many athletes – and especially in motorsport riders – the fascia is too rigid to accommodate this volume increase. The compartment behaves like a non-expandable can. Pressure rises, veins are compressed, and blood can no longer drain. Local circulation becomes an anaerobic island: oxygen-rich blood continues to flow in while oxygen-depleted blood backs up.
The cascade that follows is brutally efficient at stopping you:
Muscle contraction → volume increase → fascial tension → venous outflow obstruction → pressure rise → ischemia → anaerobic metabolism → lactate and H⁺ accumulation → pain receptors fire → loss of strength
In British Superbike riders diagnosed with arm pump, compartment pressures averaging 30.5 mmHg were recorded after a simulated braking protocol (compared with 11.7 mmHg at rest), and grip strength dropped by an average of 30% (O'Dowd et al., J Orthop Surg Res, 2021). In extreme cases, pressure peaks of up to 130 mmHg have been documented (Brown et al., J Hand Surg, 2011) – with normal blood pressure being 120/80 mmHg. At that point, sufficient capillary perfusion is simply no longer possible.
You know the result: hard, aching forearms, numb fingers, uncontrolled grip, loss of control. Fully reversible – but always at the worst possible moment.

Why Does It Hit Motorsport Riders So Hard?
There is no other sport that delivers such a perfect combination of risk factors for CECS as motorcycle racing.
Heart Rate
Motorsport is physiologically more extreme than most outsiders realize. Studies on motocross riders show that during a race, heart rate exceeds 90% of maximum for 87% of race time (Ascensão et al., J Sports Med Phys Fitness, 2008). Lactate levels rise to 5.2–6.5 mmol/l (D'Artibale et al., J Sports Sci, 2008; Simões et al., Asian J Sports Med, 2016) – on par with intense endurance competitions, with the difference that maximum fine-motor control is required at the same time.
Sustained Isometric Loading
While a cyclist varies grip rhythmically, motorcycle riding requires continuous isometric tension on the handlebars. Blood flow in the forearm begins to be restricted at as little as 10% of maximum voluntary contraction. During active front-wheel braking you work at roughly 30% of maximum grip force (Marina et al., PLoS ONE, 2021) – continuously, corner after corner.
The Vibration Factor
Motorcycles – especially singles and two-strokes – produce vibrations that trigger the so-called tonic vibration reflex. The nervous system involuntarily contracts your forearm muscles to stabilize against that vibration. You simply cannot consciously relax as long as the engine is running.
Adrenaline and the "Death Grip"
Stress activates the sympathetic nervous system, adrenaline is released, the entire body goes on high alert – and your grip tightens. This reflexive death grip is especially common in riders under pressure or in unfamiliar situations. It massively amplifies the isometric component.
Heat and dehydration round out the toxic cocktail: reduced plasma volume increases blood viscosity, which further raises flow resistance through already compressed capillaries – and an elevated hematocrit pushes heart rate into the anaerobic zone even sooner.
The Most Common Training Mistake: Muscle vs. Fascia
Now we get to the heart of the matter – the point where many well-trained motorsport athletes make a fundamental mistake.
Dutch physiotherapist Jansen from Deurne puts it succinctly: "Doordat sporters te snel hun trainingen opbouwen neemt de spiermassa te snel toe" – in English: Because athletes ramp up their training load too fast, muscle mass increases too quickly and pressure in the compartment becomes too high.
That sounds simple, but the mechanistic background is crucial: muscle tissue responds quickly to intense stimuli. Heavy strength training, intense dumbbell sessions, pull-ups to failure – measurable hypertrophy appears within 6 to 12 weeks. Fascial tissue, on the other hand, is metabolically sluggish. It adapts over months to years and primarily needs low-intensity, aerobic loading stimuli to improve its compliance.
This exact mismatch was documented by Harrison et al. (2013) in a study of elite rowers from the British "World Class Start Programme." This program took competitive athletes from other sports and fast-tracked them to Olympic rowing level. The result: several athletes developed forearm CECS because "a rapid increase in muscle bulk after reaching skeletal maturity in an accelerated training programme may have been a causative factor". Resting pressures in these rowers rose from 7–14 mmHg to 25–75 mmHg under exertion.
In the largest motocross-specific pressure dataset to date, Winkes et al. (2012) measured a mean exertional pressure of 78 ± 24 mmHg in 24 motocross riders – nearly three times the diagnostic threshold of 30 mmHg.
The paradox: The athlete who trains the hardest and builds muscle mass the fastest actively drives up packing density in the compartment. More muscle mass in the same inelastic fascial space means less tolerance for exertion-induced volume increases.
"You just need longer stringier muscles rather than clumps. It's better to be a tri-athlete than a body builder. Bodybuilders will pump up in three seconds, whereas tri-athletes can keep going." — Casey Stoner
That is not an opinion. That is physiology.
What You as an Athlete Can Do: Training Programming as the Key
If the central mistake is building up too fast and too intensely – then the solution is clear: intelligent periodization with a clear focus on aerobic capacity and capillarization.
The 80/20 Heart-Rate Principle
The most important rule: 80% of your training volume should be below the anaerobic threshold. This may sound counterintuitive for an ambitious motorsport athlete – but the physiological logic is sound:
Aerobic training at 65–78% of maximum heart rate specifically promotes angiogenesis – the formation of new capillaries in the muscle. More capillaries mean more parallel blood vessels, which lowers flow resistance and delays pressure build-up in the compartment. At the same time, lactate clearance capacity improves: lactate is channeled as fuel into aerobic metabolism rather than accumulating in the compartment.
| Phase | Content | Heart Rate | Goal |
|---|---|---|---|
| Off-Season | Running, cycling, swimming – purely aerobic | 65–75% HRmax | Capillarization, aerobic base |
| Pre-Season | Aerobic foundation + HIIT intervals | 75–90% HRmax | Build anaerobic tolerance |
| Race Season | Maintenance volume + recovery | Individual | Prioritize recovery |
Do not start a new season at maximum intensity. Give the fascia time to keep up with muscle growth.
Specific Forearm Training: Capillarization, Not Hypertrophy
The goal of forearm work is strength-endurance and vascular density – not maximum muscle size. That means:
- Wrist Curls: 3–4 sets × 20–30 reps with light weight (2–5 kg). Both palmar (palm up, flexors) and dorsal (palm down, extensors).
- Rice Bucket Protocol: 30 seconds per movement, 3 sets – dig, squeeze, stir, lever. Particularly effective for 360° forearm conditioning without a hypertrophy stimulus.
- Extensor Balancing: Rubber band around the fingers, open the hand against resistance. Riding loads the flexors heavily. If the extensors are weak, the flexors must constantly stabilize – exactly what amplifies arm pump.
- Heavy Weights: Leave them out. At least for the forearms. This is not a contradiction to hard training – it is the understanding that different goals require different methods.
- Stretching: Wrist dorsiflexion with a straight elbow, 3 × 30 seconds. No miracle cure, but an important contribution to fascial compliance over time.
Metabolism & Supplementation: The Four Metabolic Target Parameters
Beyond structural training, there are four metabolic levers that I regularly address in my work with motorsport athletes:
- Improve lactate clearance – through aerobic base training (see above). The best supplementation is useless if the aerobic system is untrained.
- Promote capillarization – Dietary nitrates play a concrete role here. Nitrates from beetroot or spinach are converted via the nitrate-nitrite-NO pathway to nitric oxide (NO), a potent vasodilator. NO is especially effective at low oxygen and acidic pH – precisely the conditions present during arm pump. One research finding shows that forearm blood flow at 45% maximum voluntary contraction increases by 585% above baseline, correlated with NO biomarkers (Lee et al., Int J Sports Med, 2000). Practical recommendation: 6–8 mmol dietary nitrate (concentrated beetroot shot) approximately 2 hours before training or racing.
- Acid buffering – Beta-alanine raises intracellular buffering capacity of muscle cells against H⁺ ions via its metabolite carnosine. The dose is 3.2–6.4 g daily for at least 4 weeks – it requires a loading period and therefore has no acute effect on race day itself.
- Inflammation & membrane fluidity – Omega-3 fatty acids (EPA/DHA, 2–4 g daily) are incorporated into muscle cell membranes, improve membrane flexibility, and reduce the local inflammatory response. Particularly relevant during ischemia-reperfusion cycles. At least 8 weeks are needed for measurable membrane effects.
Magnesium (400–600 mg daily) rounds out the basic package: Magnesium is a physiological calcium antagonist, promotes muscle relaxation, modulates ATP synthesis, and has been shown to reduce blood lactate accumulation (Nica et al., Nutrients, 2017).
An honest assessment: Supplements are supporters, not repairers. They can mitigate the metabolic bottleneck, but they cannot open an inelastic fascia. Only consistent aerobic training over time can do that – or, when necessary, a surgeon.

Holistic Prevention: Heavy Feet, Light Hands
No chapter on arm pump would be complete without the technical component. The most fundamental principle in motocross and off-road training is: Heavy Feet, Light Hands.
Your legs – knees, thighs, calves, ankles – are the primary contact surface with the motorcycle. The hands are for control, not for holding on. If you can say at a rough section that you could let go of the handlebars, you're doing it right. If you notice that you have to hold on to the bars, you're transferring work to the forearms that the legs should be doing.
Practical Techniques
- Actively press your knees against the motorcycle, shift weight through the seat
- Keep elbows high and loose – prevents shoulder and arm tension
- On straights and calm sections: loosen your grip, consciously extend your fingers and close them again
- Breath control: Box breathing before the start (4 sec in, 4 sec hold, 4 sec out, 4 sec hold) activates the parasympathetic nervous system and dampens the adrenaline spike
Ergonomics & Hydration
Lever position directly affects the gripping angle. A brake lever set too high or too low forces the wrist into an extreme position, which reduces compartment volume in advance. A neutral wrist position in the attack stance is the goal. Vibration-dampening grips and – where permitted – steering dampers reduce the reflexive death grip during unexpected impacts.
Hydration: At least 500 ml per hour at normal temperatures, more in the heat. Dehydration increases blood viscosity and drives heart rate into the anaerobic zone – both direct arm-pump triggers. Don't forget electrolytes (especially sodium) for fluid retention.
The Muscle Memory Effect
Many riders report that the first moto is significantly worse than the second. This is not imaginary. Muscle memory and aerobic activation need time. A structured warm-up on a stationary bike or jump rope activates aerobic metabolic pathways, reduces the adrenaline spike, and improves initial capillary perfusion. If you go straight into race pace without a warm-up, your body starts in anaerobic emergency mode for the first few minutes.
When It Happens Anyway: Surgery as the Last Resort
Sometimes training and prevention are not enough – especially for riders who have been racing for years with inelastic fascial structures. That is when fasciotomy comes into play.
The principle is simple: the constricting fascia is cut open (or in a full fasciectomy, removed) so the compartment has room to expand. As Dr. Angel Villamor described: "We examined the muscle fascia, which were hypertrophied and had to be opened up and released." Pedrosa's operation lasted two hours and required microsurgical precision.
The data are encouraging: In the most comprehensive systematic review to date (Gawel et al., Am J Sports Med, 2024) with 500 patients across 38 studies:
- Overall success rate: 94.2% for return to sport
- Average return time: 5.1 ± 2.3 weeks
- Recurrence rate: only 2.4%
Modern minimally invasive techniques – endoscopic fasciotomy or ultrasound-guided fasciotomy – now allow return to sport within 25 to 30 days (Facon et al., Hand Surg Rehabil, 2024).
"My first year of Moto2, I couldn't ride, I was just a passenger basically every race. So I got the surgery at the end of that season, and immediately when I jumped back on the bike, I felt like another rider." — Miguel Oliveira
This is not an advertisement for surgery – it is the reality of a truly limiting factor that was finally resolved. The operation is not the end of the road – postoperative training is just as important as the procedure itself.
Conclusion: Arm Pump Is Not a Fitness Deficit – It Is a Metabolic Bottleneck
I work with motorsport athletes who spend hours on the ergometer, log running volumes like marathon runners, and still lose their arms during the second moto. And I work with riders who don't look particularly athletic on paper but have become virtually immune to arm pump through years of aerobic base work and consistent technical practice.
The difference is not fitness in the traditional sense. It lies in understanding what the body truly needs while riding: capillary density, lactate clearance capacity, fascial compliance, and metabolic buffering. These are all qualities that develop over time with the right training stimuli – and that can be actively worsened by the wrong stimuli.
Stoner framed it as triathlete vs. bodybuilder. I put it this way: A well-trained endurance engine protects you from arm pump not in spite of its endurance characteristics, but because of them. Long, capillarized muscles with high lactate-shuttle capacity do not go anaerobic in seconds. Compact, hypertrophied type-II fibers in a tight fascial space do.
This is not an invitation to stop training hard. It is an invitation to train smart. To understand the difference between the stimulus the body needs and the stimulus the ego prefers.
If you want an individual assessment of your training program, periodization, or metabolic status – I'm here to help. Get in touch.
Sources
- Gawel RJ et al. Return to Sport After Fasciotomy for Chronic Exertional Compartment Syndrome of the Forearm: A Systematic Review. Am J Sports Med. 2024. DOI: 10.1177/03635465231216368
- Hirardot T et al. Diagnostic criteria of forearm chronic exertional compartment syndrome: a systematic review. OTSR. 2024. DOI: 10.1016/j.otsr.2024.104001
- O'Dowd D et al. Forearm compartment pressures and grip strength in elite motorbike racers with chronic exertional compartment syndrome. J Orthop Surg Res. 2021. DOI: 10.1186/s13018-021-02765-z
- Harrison JWK et al. Chronic exertional compartment syndrome of the forearm in elite rowers. Hand (N Y). 2013. DOI: 10.1007/s11552-013-9543-4
- Winkes MB et al. Long-term results of surgical decompression of chronic exertional compartment syndrome of the forearm in motocross racers. Am J Sports Med. 2012. DOI: 10.1177/0363546511425647
- Chandwani D, Varacallo MA. Exertional Compartment Syndrome. StatPearls. 2023. NCBI Bookshelf
- Ascensão A et al. Physiological, biochemical and functional changes induced by a simulated 30 min off-road competitive motocross heat. J Sports Med Phys Fitness. 2008. PubMed
- D'Artibale E et al. Heart rate and blood lactate concentration of male road-race motorcyclists. J Sports Sci. 2008. DOI: 10.1080/02640410701790779
- Simões VR et al. Neuromuscular and Blood Lactate Response After a Motocross Training Session. Asian J Sports Med. 2016. PMC
- Marina M et al. Forearm muscles fatigue induced by repetitive braking on a motorcycle braking simulator. PLoS ONE. 2021. PMC
- Facon JB et al. Ultrasound-guided fasciotomy in forearm chronic exertional compartment syndrome. Hand Surg Rehabil. 2024. DOI: 10.1016/j.hansur.2024.101719
- Nica AS et al. Can Magnesium Enhance Exercise Performance? Nutrients. 2017. PMC
- Lee SJ et al. Nitric oxide biomarkers increase during exercise-induced vasodilation in the forearm. Int J Sports Med. 2000. PubMed
- Brown JSS et al. Chronic exertional compartment syndrome of the forearm. J Hand Surg (Eur). 2011. DOI: 10.1177/1753193410397900
- MotoGP.com. Arm pump: a predominant issue for MotoGP riders. May 5, 2021. MotoGP.com
- Strang S. Stoner mystified by arm pump. Autosport. 2010. Autosport
- Fysiopraktijk Jansen. Compartimentsyndroom van de onderarm. fysiopraktijkjansen.nl
- Regas I et al. Epidemiology of upper limb CECS in French motorcycle racers. Hand Surg Rehabil. 2021. DOI: 10.1016/j.hansur.2020.12.017